About a month ago, I watched Kenyan mothers share the cost of giving birth in Kenya. This was on TikTok, where I remained glued for a couple of days as I listed to them disclose the amounts they paid to deliver their babies in different hospitals across the country.
The figures varied widely, from fees in public hospitals being as low as KSh 100, to bills as high as KSh 420,000 in private hospitals.
The differences in cost depended on several factors, including:
Whether the delivery was vaginal or via caesarean section
Whether the mother chose her own private doctors (gynaecologist and paediatrician)
The type of room selected, such as a private room
Any complications affecting the mother or baby
Length of stay in hospital
Use of private insurance
Whether SHA or other schemes covered part of the costs
How long ago the birth took place
Among the mothers who shared their costs were Wendy Gachara at MP Shah hospital, Nkatha Kobia at AAR, Dr. Selifa Kaira at Outspan Hospital in Nyeri, Cyancity_brands at Pumwani Hospital and her second at a private hospital, Teb at Nairobi Hospital, Davina at Nairobi West Hospital, ima at Avenue Hospital, and The Influenced Babe who shared the costs of her three births in different hospitals. Many other mothers shared their childbirth charges -both in private and public hospitals in the comments sections of these posts.
I found some of the charges shared by these mothers quite interesting, especially the itemised bills from private hospitals. One mother for example said she was billed KSh 350 per minute for theatre charges during her caesarean section. She spent 43 minutes in theatre.
Is safe motherhood becoming a luxury in Kenya?
The revelations by these Kenyan mothers sparked online datable, which spilled to other platforms including X and Facebook. People asked different questions:
“Has safe motherhood become a luxury in Kenya? Does having a ‘quality’ birth experience in Kenya mean digging deep into your pockets? Are Kenyan families paying for better maternal care, or are they simply paying for inflated pricing? Do higher costs translate to better maternal outcomes? Are hospitals transparent about billing? Also, why are many of these mothers on TikTok (who represent a significant portion of Kenyan mothers), delivering in private facilities instead of public ones? Have Kenyan mothers lost confidence in public hospitals and if yes, why so?”
“I was billed KSh 350 per minute for theatre charges.”
From the responses to these videos, many women thanked the mothers for openly sharing the delivery charges, especially pregnant mothers who were still hospital shopping. Women said the figures were quite eye-opening (and even frightening). Others who had thought they were ready to get pregnant indicated they were now rethinking their decisions, as they didn’t feel financially prepared anymore. Interesting, isn’t it?
My overall take is that these revelations highlight the need for decision-makers to work toward a system where every mother in Kenya can access respectful, quality maternity care without the crippling fear of hefty bills or a birth experience they do not consider ‘quality’. More importantly, Kenyan mothers need to regain confidence in the public health system because, from the comments and experiences shared, this confidence is clearly lacking.
What are your thoughts about this issue? If you are a Kenyan mother, how much did you pay for delivery? Was your delivery covered by insurance (NHIF/SHA/private), or did you pay out of pocket? Feel free to share in the comments section. If you’d like to elaborate more, you can reach me on maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
In Kenya today, conversations around HIV are more open than they were decades ago. Over the years, we’ve seen lots of advocacy, public awareness and increased access to treatment across the country -efforts that have helped to demystify many issues around HIV/AIDS. In fact, it’s no longer unusual to find people publicly sharing their HIV status on TV, radio, newspaper articles, and on different social media platforms. However, there still exist some elements of stigma associated with the disease, which makes disclosure difficult for some people, especially when it comes to romantic relationships.
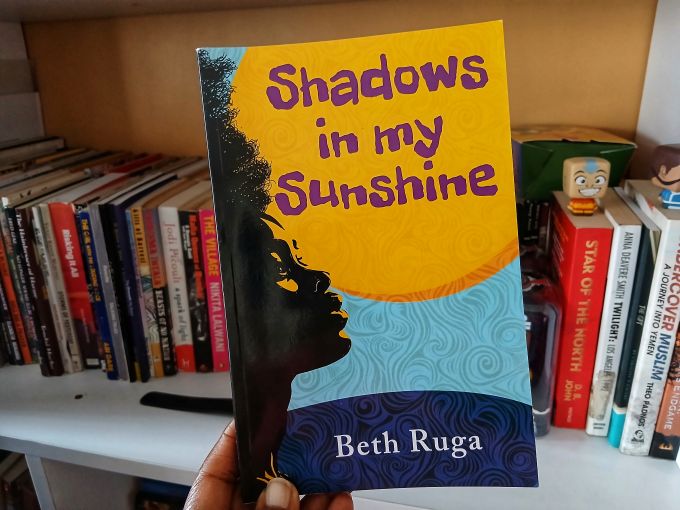
In her new novella, Shadows in my Sunshine, Nairobi-based author Beth Ruga explores these realities through the story of Wangeshi, a young woman born with HIV who must navigate romance, family, loss, her university studies, friendships and her own fears about disclosure.
Beth, 45, is a mother of three children aged 21, 13, and 10. She launched her 158-page book on Saturday 7 March 2026 at the Kenya National Library Service (Maktaba Kuu) in Upper Hill, Nairobi.
Below is my conversation with Beth about her new book.
My copy of Beth Ruga’s Shadows in my Sunshine.
Maryanne: Describe your book briefly.
Beth: Shadows in my Sunshine is about coping with HIV acquired at birth or during pregnancy, told through the love story of a young woman called Wangeshi.
Maryanne: The book’s cover is remarkable. Tell us more about it.
Beth: Yes, it is, thank you! It is the combined effort of my very good designer, Kitui Djothefu and an author’s eye for the good stuff.
Maryanne: What inspired you to write Shadows in my Sunshine, and why did you choose to center the story on a young woman born with HIV?
Beth: As you may already know, new HIV infections are on the rise in Kenya. It felt to me that people needed reminding, and I answered the call. Why a woman? I like to build my stories around women and children as they often get the short end of the stick in matters equality.
Maryanne: What does the title of the book symbolize in Wangeshi’s journey?
Beth: The Sunshine symbolises her life while the Shadows are the hurdles she has had, generally amplified by her health status.
Maryanne: The book explores the difficult decision of disclosing one’s HIV status in romantic relationships. Why was it important for you to address this theme?
Beth: Through research, I encountered many such cases and one way of demystifying the status quo would be to talk about it, so I did.
Maryanne: What do you hope young readers -especially those facing health challenges take away from Wangeshi’s journey?
Beth: I hope that young people embrace their situations, take charge of their lives by bettering themselves while staying true to treatment and living responsibly.
Maryanne: What conversations do you hope the book will spark among families, friends, people involved romantically, and the community in general?
Beth: Actually, I hope it generates as many different views as are possible. Most times, the story/book is wiser than the creator/author and takes on it’s own life. Generally, though, I hope it educates people on the need to be sensitive to people and issues that are not considered the norm, including persons living with HIV, and to exercise caution and social responsibility in their sex lives.
Maryanne: The novel highlights some aspects of Gikuyu words, practices and customs. Why was it important to weave these cultural elements into the story?
Beth: Gikuyu is my indigenous language and I like to sprinkle it, for lack of a better word, in my writing to pay homage. I don’t even provide a glossary for the same, but I ensure the words used do not lose the reader, especially the non Gikuyu speakers. It is basically a style of choice.
Maryanne: Do you think conversations around HIV/AIDS have changed since the disease was officially declared a national disaster in 1999? If yes, how so?
Beth: Yes, greatly. People are talking about it more, publicly declaring their status and even publicly taking treatment, which is good. On the flip side, it seems like the disease has been around too long and the familiarity has bred complacency, leading to recklessness in sexual behaviour.
Maryanne: If readers are to remember one message from Shadows in My Sunshine, what would you want it to be?
Beth: That we may have won the battle with HIV/AIDS when treatment was discovered, but the war is far from over.
Maryanne: How long did it take you to write this book?
Beth: I lose track most times, but approximately a year and a half to two years.
Maryanne: Did writing this book change you in any way, or make you realize something about yourself that you didn’t know before?
Beth: I always knew I could weave a good short story but writing a novella was something that was a good surprise!
Maryanne: What has the response been like so far from readers?
Beth: It has been awesome. The reception has been amazing. I look forward to the book reading to hear and address the reactions of my readers.
Maryanne: What are you working on next?
Beth: I’m working on a Young Adult investigative story.
Maryanne: Congratulations Beth on your new book and looking forward to reading your next one.
So there you have it. I hope you’ve gotten a glimpse of Beth’s book through her own words. Shadows in my Sunshine is an easy read, and I encourage you to get yourself a copy and indulge in the world of Wangeshi, where you’ll experience life from the point of view of a young woman navigating family affairs, friendships, relationships and HIV disclosure (and marriage too!).
Have you read the book already? What are your thoughts about it? If you haven’t, please do let me know your thoughts about it 😊
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
Is it safe to have a tooth extracted when pregnant? A family in Nairobi is demanding answers after 28-year-old Viona Munai, who was nine months pregnant and preparing to give birth, died following a dental procedure to treat a tooth infection. Her unborn baby also did not survive. My sincere condolences to her family and friends. Such a young life gone too soon.
Viona’s unfortunate incident however raises such an important question: should a pregnant woman have a tooth extracted? Or is it usually safer to wait until after delivery?
This is a question that confuses many pregnant women, those planning to be pregnant, or mothers in general -myself included. We are always confused with no clear answers, even from medics themselves who offer conflicting views. We are always given all manner of advice, scares and encouragements about tooth extractions when pregnant, only adding to our uncertainty about the procedure. You only need to see the comments to that video about Viona, and you will understand what I mean. Let me sample some of them below:
“I had a bad cavity when I was pregnant and doctor’s told me they can’t extract when a woman is pregnant. I relied on panadols all through. So this was Soo wrong
“Pregnant women are not extracted teeth. Doctors advice Is to wait until you deliver.”
“You don’t extract a tooth of a pregnant lady.”
In another forum, one pregnant woman asked it if was safe for her to have her tooth extracted, and tens of women responded. Some shared their personal experiences, others shared advice based on what they have heard. I will sample some of them below:
“I had a bad toothache and a dentist advised against extraction since I was 12 weeks pregnant. I tried my best but couldn’t bear the pain anymore, so I went to another clinic, didn’t say I was pregnant and they extracted the tooth. I thank God everything went well.”
“I suffered for three months since I was in my third trimester and the doctors advised against extraction. I survived on antibiotics and paracetamol.”
“The pain I was having was terrible so I had my tooth extracted. However, after two days I miscarried. I can’t say it was because of the extraction and neither can I say it wasn’t, but never again.”
“I had heard that we are not supposed to have teeth removed, but when I was 8 months pregnant I couldn’t cope with the ache, I was unable to eat and I was having a headache throughout because of the pain so I went and had it removed. I had no complications.”
“In my case I was advised against it cos of the blood pressure levels I had at that time.”
“Mine was extracted when I was 8 months pregnant because after a week of pain I was almost going mad… I couldn’t take it anymore, I got it removed.”
“I was 7 months pregnant when I had my tooth extracted. The following month I went into premature labour and had a still birth. I don’t know if the two are related.”
The toothache pain I went through was too much, in fact I got two of them extracted. I was like if I die, I die because either way the pain was already killing me anyway.”
Mine was extracted at 6 months pregnant and I was given antibiotics in case of any infection. You just need a proper dentist. Gone are the days people used to say a tooth cannot be extracted when pregnant. Does it mean if your tooth is problematic at month 2 you will be on painkillers for the next 7 months?
“I got mine extracted at 8 months after being on a lot of strong painkillers but the pain was still unbearable. I took the risk.”
More women shared their experiences:
“Mine was extracted at 5months…no complications.”
“I got mine removed when I was 25 weeks and didn’t experience any issues.”
“Mine was extracted at 7 months. No complications.”
“I did when I was 6months on my first pregnancy. No issues.”
Others offered their advice:
“Think twice before extraction. the injection you get before the tooth pulling can cause miscarriage.”
“Get calcium supplements to push you till delivery coz most tooth problems are escalated by pregnancy.”
“Get some cloves powder, mix with water and paste the mixture on the aching tooth. That is how I treated mine.”
“Drink a lot of milk to boost your calcium, then wait until after delivery to have it extracted.”
“Talk to your gynaecologist and your dentist. Just because someone else did it and nothing happened to them doesn’t mean it’s safe.”
“It is not advisable. If you can wait till after delivery, please do.”
“There are no contraindications unless you have underlying medical conditions.”
More confusion
All these comments only add to the confusion and a woman is left wondering what the right decision is. Can you imagine what a pregnant woman is supposed to do when she is in immense pain, and the tooth extraction seems like the only way out? If you have ever had a toothache, trust me, the pain is usually on another level. I don’t ever wish that kind of pain on anyone. So what is a pregnant woman supposed to do?
What has been your experience, or that of a woman you know? In case you have a ever had a tooth removed while pregnant,
How many months pregnant were you?
How was your experience?
Were you given any warning or advice before the extraction?
Do you think there should be more clear guidance about tooth extractions for pregnant women?
I would really like to hear your thoughts. You can share in the comments below, or you can email me on maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
21 year-old Valerie Kasaya is 5 foot tall. While attending her antenatal clinics, the nurses had told her that there was no way she was going to give birth naturally. Reason? She was too short. They were blunt like that. Well, Valerie’s mother could hear none of that, and she decided to take her daughter to a different health center where she would be encouraged to try have a vaginal birth first, and if not, then a c-section.
When labor came, Valerie trekked to a little health facility in Kawangware called FreMo clinic and with the help of a midwife, she safely delivered a healthy 3.1kg baby. It only took four hours of labor. Valerie did not have any complications, no episiotomy, no nothing. It was a smooth delivery for this first-time mother.
A beaming Valerie with her son.
It is encouraging to know that is possible for short women to give birth vaginally. A short woman should not automatically be written off for vaginal delivery purely on the basis of her height. Valerie is one such example. She and her son, who is now eight months old continue to enjoy robust health.
However, in some cases, there are short women who are not able to have vaginal deliveries. And in the same breath, there are also big women who cannot give birth naturally. Height is not the sole determinant for this.
I spoke to Dr. Stephen Mutiso, a consultant obstetrician / gynaecologist who explained it to me very well. According to him, a diagnosis of cephalo-pelvic disproportion (CPD) is what determines if any woman –whether short or tall, will give birth naturally or via caesarean section. Cephalo refers to the size of the baby’s head, and pelvic means the size of the birth passage.
A diagnosis of CPD means that either the baby’s head is too big for the woman’s pelvis, or the pelvis is too small for a normal sized baby. In women diagnosed with CPD, natural delivery is difficult and at times impossible.
Dr. Stephen Mutiso
“Small women tend to have a small pelvis, and are likely to have difficulties during delivery. Any woman with a small pelvis and whose baby indicates being slightly bigger compared to her pelvis is not advised to try normal delivery,” he says.
However, Dr. Mutiso clarifies that there are short women who have small babies and go on to have successful normal deliveries, and that is why it is important for the doctor, nurse or the health professional attending to the pregnant woman to do a proper assessment –during pregnancy or when labour begins.
This assessment helps determine if the pelvis is adequate enough to allow baby to pass through. If the baby’s size is small to average, then labour should be considered.
The health facility in Kawangware where Valerie delivered her son.
For women who insist on pushing a baby that cannot pass through a small pelvis, Dr. Mutiso warns of the consequences.
“This could lead to prolonged labor and cause obstruction, which in turn may result in complications such as fistula, rupture of the uterus, serious infection, foetal distress and excessive bleeding after birth. In some instances both mother and baby may die.”
He goes on to say that in the event vaginal delivery goes on to take place, the mother can sustain serious perineal tears or cause damage to her reproductive organs. Further, caesarean deliveries done when one has been trying to push are more difficult and associated with increased complications.
So, in as much as most pregnant women plan to delivery naturally, it is important to understand that complications may arise during labour, and which may necessitate a caesarean section. These complications include; failure for labor to progress despite good contractions, foetal distress and excessive bleeding.
The good thing to know though is that there are short women who can have natural births, Valerie being a good example. But, be adequately informed about the same. Knowledge is power. Talk to your doctor, and make sure a proper assessment is done. If are certified to do so, then is all good, but do not insist on trying to do something that may cause you or your baby dire consequences.
Do you have a birth story to tell? If you’d like to share your story, email me on maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
Last week, I shared the story of Diana A. Otieno, who wrote about her experiences as a mother to a premature baby, and even went on to author a book about that journey. (You can catch my interview with Diana here.) It is therefore interesting, and quite timely, that I have come across yet another uplifting story of prematurity, this time from Kenyatta National Hospital (KNH), which I’m sharing below.
When Vivian Anyango became pregnant for the third time, she carried with her a deep hope that this time, she would make it to term. She and her husband, Kenneth Otieno, had previously lost two pregnancies, so the joy of expecting again was inevitably accompanied by anxiety and fear.
Things seemed to be going well. Until they weren’t.
Going into labour at 25 weeks
At just 25 weeks into the pregnancy, Vivian went into labour. One can only imagine how terrifying that moment must have been for the couple. Were they about to lose yet another pregnancy? On 26 September 2025, Vivian was referred to Kenyatta National Hospital in Nairobi, where a team of doctors and nurses worked tirelessly to stabilize her and prepare for the journey ahead.
Four days later, Vivian delivered extremely premature twins. Twin One weighed 750 grams, while Twin Two weighed just 650 grams. Their lives began in the Newborn Unit (NBU), which would become their home for several months as they fought to survive.
Both babies were placed on Continuous Positive Airway Pressure (CPAP) machines to help them breathe. Their survival depended on specialized medical care, constant monitoring, and the unwavering commitment of their parents. Vivian practiced Kangaroo Mother Care, which is a recommended method for caring for preterm babies that involves prolonged skin-to-skin contact. In this case, Vivian was caring for two tiny babies at once.
Active father involvement in premature birth care
Kenneth, too, showed up every single day. For four months, he was consistently present and actively involved in his babies’ care. He even provided Kangaroo Mother Care himself. This highlights the powerful role that fathers play in maternal healthcare, especially during moments of fragility.
But the journey was far from easy. At one point, the twins’ weights dropped to a frightening 550 grams and 500 grams. But through the dedication of the KNH medical team and lots of breastfeeding, hopes and prayers, the babies slowly began to gain weight. Grams turned into more grams, lifting the spirits of the parents and the medical team.
Walking out of hospital as a family of four
By the time they were ready for discharge, Twin One weighed 1,830 grams, while Twin Two weighed 1,790 grams. This was such incredible progress from their earlier weights of 750 grams and 650 grams.
Finally, on 20 January 2026, after more than four months in hospital, Kenneth and Vivian walked out of Kenyatta National Hospital with both their babies alive and well. Their journey also marked a historic milestone: it is the first documented case at KNH where extremely preterm twins were delivered and survived to discharge.
The couple and part of the medical team at KNH. Photo courtesy: Kenyatta National Hospital.
This is such a warm, encouraging, and uplifting story. Congratulations to the KNH team, and to Vivian, Kenneth, and their twins. Here at Mummy Tales, we share stories like this because they matter. Because behind every preterm statistic is a parent hoping against hope, babies fighting for their lives, and medical teams who similarly do their best for positive outcomes.
We wish Vivian, Kenneth, and their beautiful babies continued good health and a future filled with many joyful milestones.
Do you have a premature birth story to tell? If you’d like to share your story, email me on maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
Diana A. Otieno is a 36-year-old mother of two boys aged 4 and 10 years. An entrepreneur based in Nairobi, Diana recently published her new book titled: ‘The Strength We Share: Lessons and Miracles from the World of Prematurity’ which captures her journey as a mother of a premature baby. In the book, she also weaves in the experiences of other Kenyan mothers who have walked the same path with their preemie babies.
When I finished reading the book, I immediately knew that I wanted to share more details about it with my Mummy Tales readers. It was an easy, short read which I completed in just under two hours. As I turned the pages, I found the stories to be quite relatable, as in them, I could recognize the experiences of people I know -my relatives, colleagues, friends, and neighbours. This is a book that any mom would find comforting and uplifting, and I encourage you to consider getting a copy for yourself or gifting it to someone who needs the encouragement, especially a preemie mom.
Beyond the stories, I was also curious to learn more about Diana herself. I wanted to know more about what inspired her to write this book, and what she hopes it will achieve.
The book costs KES 1,000. You can get it from Nuria or Kibanga bookstores, or you may order it directly from Diana on +254 740 845 798.
Below is my short interview with Diana.
Maryanne:What inspired you to write this book?
Diana: ‘The Strength We Share: Lessons and Miracles from the World of Prematurity’ was inspired by my journey with my son and our time in the neonatal intensive care unit (NICU). It was a deeply traumatizing experience but through it, I began to heal and recognize my own strength. I wrote this book to remind NICU mothers that they are not alone and to share the stories of others, highlighting the resilience, courage, and strength we share. Today, my 10-year-old son is thriving, and that remains my greatest victory.
Diana A. Otieno’s sons playing together in a recent photo.
Maryanne:When did the idea first come to you?
Diana: The idea had been on my mind since 2017, but at the time I didn’t feel worthy of sharing it. I struggled with imposter syndrome and was still navigating life as a new mother. In 2024, I revisited the idea more intentionally. I began writing my own story and later felt compelled to include the stories of other mothers as well, realizing that our shared experiences were meant to be told.
Maryanne: What were some of the biggest challenges you faced as a preemie mom?
Diana: One of the biggest challenges was the emotional and mental toll, the constant fear, guilt, and uncertainty, especially as my son’s heart condition and later speech delays deeply affected my mental health and made me feel like I had failed him. Physically, recovery was demanding, while societal judgment added another painful layer, with people making harsh assumptions without understanding my reality. Financially, managing his medical needs, particularly his heart condition, was extremely draining.
Maryanne: What kind of support made a difference for you at that time? What support do you wish had been more available?
The support that made the biggest difference for me came from other mums in Preemie Love, a support group of women who truly understood the journey. Support also came from my family, who have been unwaveringly supportive. What I wish had been more available is consistent psychosocial support for NICU mothers, so that even after leaving the hospital, someone could follow up, visit, and assist with feeding, bathing, or general care. Imagine being at home as a first-time mom with a 1.8 kg baby; it can feel completely overwhelming without that kind of hands-on support.
Maryanne: As a preemie mom, what small wins have given you strength along the way?
Diana: My son started talking at five years old, which has been the greatest victory of all. With speech came independence, better understanding, and less worry about him wandering off, making everyday life so much easier.
Maryanne: Why did you feel it was important to share your journey publicly?
Diana: I felt it was important to share my journey because silence often makes pain heavier. Many NICU mothers suffer quietly, feeling unseen and misunderstood, and I wanted my story to remind them that they are not alone. By speaking openly, I hoped to challenge the stigma around premature birth and turn my personal healing into a message of collective strength—the strength we share.
Maryanne: What did writing your story do for you?
Diana: Writing my story was deeply healing. It allowed me to process the pain, fear, and trauma I had carried for so long, and to acknowledge my own strength in ways I hadn’t before. It brought clarity, helping me make sense of the journey and see how far we had come. Sharing it also gave me a sense of purpose, knowing that my experiences could inspire and comfort other NICU mothers.
On the left is Diana holding her preemie son.
Maryanne: Why did you feel it was important to include stories from other mothers of preterm babies?
Diana: I felt it was important to include stories from other mothers of preterm babies to show that my experience is not isolated. Including their journeys highlights the shared struggles, resilience, and strength of NICU mothers, reminding everyone that no one has to face this journey alone.
Maryanne: How did you select the mothers whose stories appear in the book?
Diana: I did so by reaching out through Preemie Love WhatsApp groups, inviting NICU mums who were willing to share their experiences. I also personally reached out to friends with whom I had walked the preemie journey. In total, I featured 10 mothers whose stories reflect a range of experiences and challenges.
Maryanne: What do you hope readers can understand about preterm motherhood through these shared voices?
Diana: I want readers to understand that prematurity is nobody’s fault and that we should extend grace to NICU mothers and those with special needs children. Instead of constantly judging other mothers as inadequate, we should recognize the challenges they face and honour the strength and resilience required to care for their little ones.
Maryanne: What message would you give to a mother who is currently going through the NICU experience?
Diana: I would say to them: you did nothing wrong, and you have not failed your child. You are not alone. Hold on to hope, even in the hardest moments. Love your child no matter what, because it is from that love that they draw the strength to survive and thrive.
Maryanne: If your younger self, who was still in the thick of the NICU journey could read your book today, what do you think she would feel?
Diana: I think she would feel seen, understood, and less alone. She might also feel a sense of hope and reassurance, knowing that the pain and struggles she was going through would eventually lead to healing, growth, and strength. Most of all, I believe she would feel proud of how far we have come.
Maryanne: How has your premature journey shaped you as a mother?
Diana: My premature journey has taught me so much and shaped me into a more informed and attentive mother. I have learned about the conditions that can arise from prematurity and the importance of asking doctors questions and doing my own research to make informed decisions. With my second child, I knew so much that doctors sometimes thought I was a medic. I have also learned to support other mums by helping them recognize signs that may require medical attention in their children.
Maryanne: Have you heard from readers so far? What responses have touched you?
Diana: Many readers have told me that my book made them cry and that some of the stories were very sad. Yet, they also said the stories gave them a new perspective on motherhood and the challenges some mothers face. For some readers who had never encountered a preemie mom, the stories were deeply touching and emotionally moving. Even my own mom suggested that my next book should be about something happier, because writing this one was honestly very depressing for me.
Maryanne: What do you hope this book contributes to the conversation around maternal health and prematurity in Kenya?
Diana: I hope this book contributes to the conversation around maternal health and prematurity in Kenya by raising awareness about the realities NICU mothers face, both in and out of the hospital. I want it to challenge stigma and judgment, highlight the need for emotional, psychosocial, and financial support, and inspire more empathy and understanding for mothers of preterm and special needs children. Ultimately, I hope it encourages a culture of care, grace, and shared strength for all mothers.
I would also like mothers, families, and healthcare providers to take away the importance of empathy, understanding, and support. Every NICU journey is unique, and even small gestures of care can make a huge difference. To mothers, I want them to know they are not alone and that their strength matters. To families and healthcare providers, I hope my story highlights the need for patience, grace, and consistent support for both the child and the mother, even long after leaving the hospital.
Maryanne: Where can we get your book ‘The Strength We Share: Lessons and Miracles from the World of Prematurity’?
Diana: People can get my book from three platforms:
Diana: Thank you for choosing to share my story. I am deeply honoured that my journey and the experiences of other NICU mothers can reach and inspire others.
So that’s a little bit of Diana and her book. Thank you Diana for taking the time to speak with me and allowing Mummy Tales to spotlight your meaningful work.
Are you a Kenyan woman author who would like to be featured on the Mummy Tales blog? You may write to me at maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
As 2025 ends, I want to take a moment to reflect on one of the most meaningful projects I’ve worked on this year -the Wanjiku Kumbukumbuseries by Mummy Tales. In this series, I shared the names and faces of some of the Kenyan mothers who tragically lost their lives during pregnancy, childbirth, or shortly after giving birth this year. What remains clear from these women’s stories is that even in this day and age, maternal mortality is still a very real and painful reality in Kenya.
The Kenyan mothers whose deaths came too soon in 2025 had different backgrounds and profiles. Some were young mothers, first-time-mothers, experienced mothers, career women, homemakers, businesswomen… We got to learn about what happened to them through the words of their husbands, mothers, fathers, sisters, friends, colleagues, and relatives. Sadly, most of these deaths were preventable. Today, their families are still grieving, wondering what went wrong and what could have been done differently.
The late Vanessa Wanjiku. Photo: Screengrab – K24TV
Each story in the Wanjiku Kumbukumbu series not only helped to raise awareness about maternal health, but also reminded us that behind every statistic is a woman who had life going on for her, a family that loved her, and dreams she wanted to achieve. She had a bright future which sadly, ended rather prematurely.
The reasons why Kenyan mothers died
Every day, 13 women in Kenya lose their lives to pregnancy-related complications. A number that is too too high. This is despite decades of interventions which include government programs, advocacy and thousands of NGO projects. Through the Wanjiku Kumbukumbu series, I captured the stories of:
Mothers who bled to death after delivery (post-partum haemorrhage)
Mothers who didn’t survive high blood pressure complications (preeclampsia)
Mothers who didn’t survive caesarean section complications
Mothers who died because of delays in accessing quality care (even within the hospital)
Mothers whose families are still searching for answers
Below are the women whose names and faces that I captured in the Wanjiku Kumbukumbu series in 2025. Their stories represent those of other mothers who lost their lives this year.
Docras Nzisa (25) who succumbed to caesarean section complications
Beyond 2025, I will continue with the Wanjiku Kumbukumbu series because I believe that continually raising awareness about maternal health through storytelling is important. It keeps reminding us of the gravity of the situation, in the hope that we can do better for Kenya’s mothers because every woman deserves to survive childbirth. I hope that the stories will:
Show that maternal deaths are not just about statistics. This is because behind each number is a beautiful woman who has left behind a huge gap
Get people to act on matters that will ensure that fewer families experience the pain that comes with losing a mother to childbirth complications
Inspire collective advocacy and accountability in our health systems, policy spaces, in our families and in the communities. Especially considering that most maternal deaths are preventable
Many thanks to every reader who followed this series, made a comment, shared the articles, reached out with information, or simply took a moment to reflect. Your reading, sharing, and engagement throughout the year helped amplify the voices of these women and their families. Thank you for being part of this journey and for supporting the Wanjiku Kumbukumbu project.
As we step into a new year, I pray that we will carry the memory of these mothers with us. I hope that their stories will strengthen our resolve to ensure that future mothers will live to raise their children.
I invite you to join me in this journey. If you would like to support the Wanjiku Kumbukumbu project, please reach me on maryanne@mummytales.com
Sincerely, Maryanne W. Waweru –Founder,Mummy Tales
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
Nancy Wanjiru Waithaka. Photo: Kenyatta National Hospital.
Pregnancy is often described as a beautiful journey, but for some women, it can also be one filled with fear and uncertainty. This is Nancy’s story, which will give hope to any woman going through a difficult pregnancy journey.
When 15-week pregnant Nancy Wanjiru Waithaka was admitted to Kenyatta National Hospital (KNH), she was battling not just an ordinary pregnancy complication, but a rare and dangerous condition known as bilateral pheochromocytoma.
Bilateral pheochromocytoma is a tumor that causes dangerously high surges of adrenaline –the kind that can push blood pressure to life-threatening levels. For Nancy, this diagnosis was saddening. The condition did not only threaten her life, but also that of her unborn baby. However, she was determined to fight for her baby. Thankfully, the team of medics at Kenyatta National Hospital (KNH) were, too.
Life-saving care at Kenyatta National Hospital (KNH)
Nancy’s treatment included care under a multidisciplinary team of specialists from KNH’s materno-fetal unit, urology care, endocrinology, and cardiac anaesthesiology departments.
For six months, they walked with Nancy in her treatment journey. The medical care included balancing her hormonal levels, controlling dangerous blood pressure spikes, and closely monitoring both she and her baby through several ICU stays.
Then, at 26 weeks of pregnancy, the doctors performed a complex and delicate surgery that included removing the adrenal tumors (one partially, one completely). It was a risky procedure, but one which was necessary to save her life and her baby’s.
A miraculous birth
Finally, after months filled with great tension, months of close monitoring and round-the-clock care, Nancy safely delivered her baby boy through a Caesarean section at 33 weeks and five days.
Holding her little one for the first time was a moment she will never forget.
“I was blessed with my boy, and so happy to see him and hold him. It’s a miracle,” she said with a radiant smile.
Today, both mother and baby are doing well. Congratulations to Nancy and the dedicated team of doctors and support staff at Kenyatta National Hospital who made this miracle happen.
May her story inspire every pregnant woman having a difficult pregnancy. May your journey end well, just like Nancy’s.
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER
In today’s digital age, it is very important that children learn how to effectively communicate with a computer which in other words, is called ‘coding’. And the earlier they learn how to code, the better for them since it sets them up for their future success -both in academics, their life skills, and in the workforce.
So, I thought of putting together a list of coding schools in Nairobi where your children can access coding skills. This list is not exhaustive, so if there’s any that I’ve left out you can let me know in the comments section below and I’ll add it.
Class Measures Limited (Kevin Muriuki) 0712 675 858
Ndehi Karonjo 0722 734 085
Did I miss out on others? Leave their names, links to website and telephone number in the comments section below and I’ll update the list. You can also email me on maryanne@mummytales.com
NB: This post has been updated from the original one published in 2021.
Mummy Talesis a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l INSTAGRAM l TWITTER
The late Dorcas Nzisa Kariuki. Photo -screengrab: Kerax Media Production.
This article highlights the maternal death of Dorcas Nzisa Kariuki, a young Kenyan mother who passed away after developing complications from a caesarean section delivery. This is story 12 in the Wanjiku Kumbukumbu series by Mummy Tales, an initiative that is documenting maternal deaths in Kenya.
Dorcas Nzisa Kariuki was born on 26 July 2000 in Kauwi, Kitui County. Sadly, Dorcas passed away on Sunday, 31 August 2025, after developing complications following a caesarean section. Though she successfully delivered her second child -a beautiful baby girl, Dorcas, unfortunately, did not make it.
Dorcas was a young mother who was full of ambition and purpose. Through her blog, Mdosi Online, she used her voice to inform, inspire, and empower others, touching the lives of many with her words and positivity. Dorcas had a bright future, with so much to achieve. Sadly, childbirth complications took her away.
Maternal deaths in Kenya
Every day, 13 Kenyan women die from pregnancy-related and childbirth complications. But these women are more than just numbers in a report. They are daughters, sisters, friends, and mothers. They are women with dreams, laughter, and love. Women like Dorcas, who had so much more life to live.
It shouldn’t be this way though. No woman should lose her life while giving life. So let’s continue to raise awareness, demand better maternal healthcare, and support initiatives that ensure every woman in Kenya can experience safe pregnancy and childbirth.
Documenting maternal deaths in Kenya
The unfortunate death of Dorcas is the twelfth account in the Wanjiku Kumbukumbu series by Mummy Tales,an initiative that is focused on documenting maternal deaths in Kenya to raise awareness about the issue and advocate for better maternal health. The project aims to memorialize Kenyan mothers we have lost to childbirth complications.
If you would like to share information about a mother who has lost her life due to maternal health complications in 2025, or if you would like to support the Wanjiku Kumbukumbu project by Mummy Tales, please reach me at maryanne@mummytales.com
Mummy Talesby Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan momshere. Connect with Mummy Tales on: FACEBOOK lYOU TUBE l TWITTER




")















")








 Mummy Tales by Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan moms here. Connect with Mummy Tales on: FACEBOOK l YOU TUBE l TWITTER
Mummy Tales by Maryanne W. Waweru is a platform dedicated to empowering its readers on different aspects of womanhood and motherhood. Read more motherhood experiences of Kenyan moms here. Connect with Mummy Tales on: FACEBOOK l YOU TUBE l TWITTER